What is the structure and location of the menisci?
There are two menisci or ‘shock absorbers’ in the knee. These are made of a tough leathery material composed of fibro-cartilage which is a mixture of collagen fibres, elastin, and a mucopolysaccharide called chondroitin sulphate. The fibres are arranged in a semi-circle firmly attached at each end and also attached at the outer edge. The menisci are quite thick towards the periphery of the joint tapering to a fine feather edge centrally giving them a crescentic appearance.
|
|

|
|
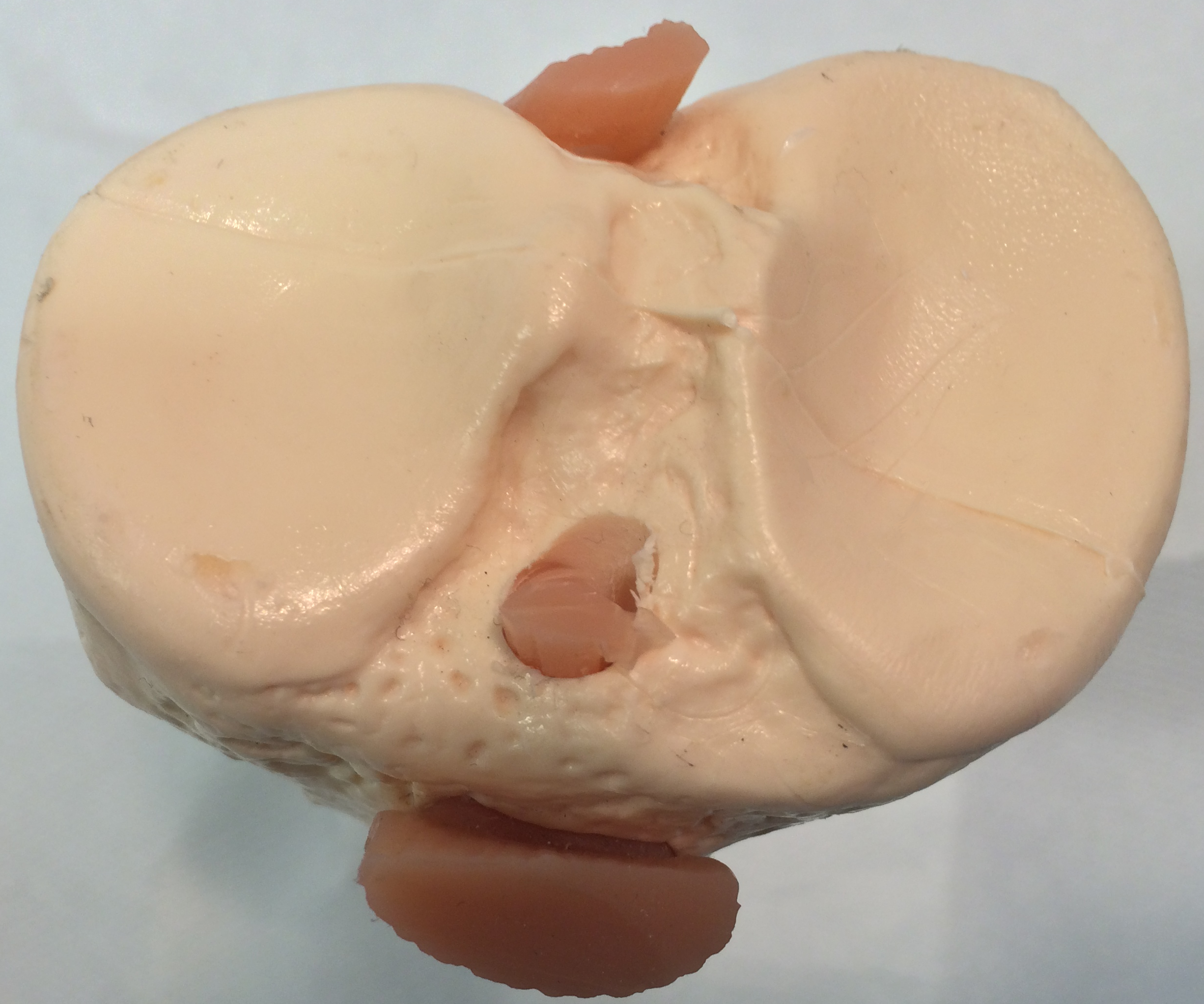
Upper tibia with the menisci removed
|
Upper tibia showing the menisci
|
Why are the menisci so important?
There are a number of reasons:
-
To absorb impact and transfer some of the load from the tibia to the femur
-
To provide extra stability to the knee alongside the ligaments
Other roles may include:
-
Proprioception and position sense through their peripheral nerve supply
-
Distributing natural lubricants and nutritional products
|
|
|
|
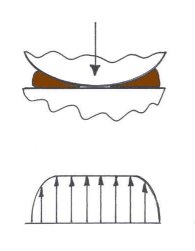
Diagram of knee with meniscus in place. Forces distributed over a broad area
|
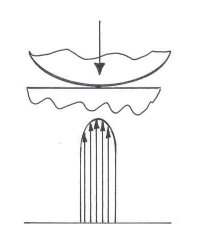
Diagram of knee with meniscus removed. Forces transferred in a narrow band
|
What are the reasons for meniscal tears?
Broadly there are two mechanisms – injury and degenerative change.
In younger people with normal menisci quite large forces are required to tear the meniscus. This usually happens in a twisting injury on the load bearing flexed knee. Such tears often happen during sports including football, rugby, netball, tennis, skiing and many other sports even golf.
Typical symptoms:
-
Initially great difficulty in walking often with acute pain
-
Aching and tenderness at the site of the tear at the joint margin
-
Giving way of the knee often accompanied by momentary sharp pain
-
Swelling due to production of extra fluid within the joint
-
Locking or jamming often preventing the knee from extending quite fully
Diagnosis:
In most cases an accurate diagnosis can be reached from the history and findings on examination. However in most cases it is important to have an MRI scan to confirm the diagnosis and to exclude other abnormalities. Neither clinical diagnosis nor MRI are 100% accurate and some meniscal tears are only revealed during arthroscopic examination. In cases where the history suggests degenerative changes plain x-rays may also be performed. These can be obtained rapidly and can be done with the patient standing revealing evidence of narrowing of the joint space and bony spurs.
|
|
|
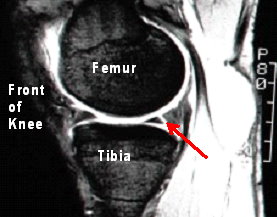
Side view of a knee with a tear at the back
of the outer meniscus shown on MRI
|
Treatment:
Minor tears frequently settle spontaneously without treatment. The younger the patient the greater is the potential for healing. Reducing the rotational forces across the knee during healing is important and physiotherapy to maintain muscle power and stability is of considerable help.
In older people with degenerate tears who have relatively less acute discomfort quite a prolonged period of conservative (non-surgical) management is also appropriate.
|

|
|
Torn meniscus seen at arthroscopy
|
The location of tear that is most readily repairable occurs in the periphery of the meniscus near to or within that part of the meniscus with a blood supply and usually of the type known as a “bucket handle tear”. The meniscus only has a blood supply right at the outer edge where it joins the capsule of the joint. This meniscocapsular region usually heals well when sutured. Indeed tears in this area have been shown to heal quite well spontaneously as long as both surfaces of the torn meniscus are in apposition and are not displaced.
The majority of meniscal tears that require surgery are unsuitable for repair and the preferred option is removal of the torn fragment and rounding off the ragged edges. It is important to carry out conservative volume sparing surgery, that is, to removal only as much as is necessary to preserve as much of the shock absorbing capacity of the meniscus as possible. This is important to prevent or reduce the chances of arthritic changes occurring later in life.
A number of scientific studies have been carried out on the use of synthetic materials to replace all or part of menisci with collagen scaffolds. These studies are ongoing and this method of treatment remains limited to a relatively few centres. Where the entire meniscus has to be removed in a young person a meniscal transplant can be carried out using cadaveric material.
Lastly tissue engineering that grows new replacement tissue for the menisci continues to be investigated and remains under development.
TEXT Copyright London Knee Clinic ®2014