Many years ago when surgeons first started operating on the menisci their importance was not appreciated. As a result, before the days of arthroscopic surgery, open meniscectomies were often carried out removing all or a large portion of a meniscus. This gave good to excellent results in the short term but if the meniscus was removed completely in a young adult there was found to be a substantially increased risk of osteoarthritis of the knee later in life. The greater the amount of meniscus removed, the greater the risk of osteoarthritis. As a result of this realisation, conservative or what we call volume sparing meniscal surgery has been the norm for many years. The aim is to remove as little of the meniscus as possible and always to repair rather than resect if at all possible.
|
|
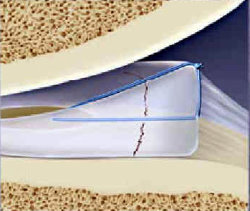
A vertical tear in a meniscus
repaired with a meniscal suture
|
Unfortunately meniscal tears are not always possible to repair. This is especially the case where the meniscus has become degenerate and where there is already early osteoarthritis of the knee joint in question.
Results of meniscal repair:
Various instruments have been manufactured to facilitate repair of menisci including suture devices that can be inserted through tiny arthroscopic incisions into the knee joint. Meniscal arrows are short absorbable rods that lock into the tissue and can be used to securely hold the edges of a meniscal tear together. As with all tissue repairs, the surgical repair is only a temporary measure while the tissue heals. The average success rate for meniscal repairs is 90% reducing significantly in older age groups. As always we are dependent on the patient’s healing response to firmly attach the torn edges. This healing response declines with age so that the results of meniscal repair are progressively poorer as we get older.
 |
Smith & Nephew Fast-fix meniscal suture
The suture is attached to two plastic achors with a slip knot
|
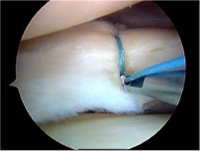 |
Meniscal suture being
inserted
using the Fast-fix system
as seen arthroscopically
|
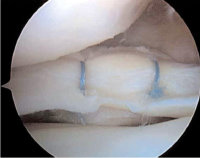 |
A bucket handle meniscal
tear
repaired using two
Fast-fix sutures
|
Protocol after meniscal repair:
- Initially: Gentle walking with crutches partially weight bearing. Remove the Gamgee pad after 48 hours. Maintain quadriceps and hamstring muscle power with static strengthening from the beginning.
- Weeks 1 to 6: Continue crutches, partially weight bearing. No knee flexion beyond 45 degrees. Continue static quadriceps and hamstring exercises.
- At 6 weeks: Gradually wean off crutches and increase knee flexion progressively to 90 degrees over a two week period. Full weight bearing is re-established. The range of motion is gradually improved non-weight bearing.
- At 12 weeks: Gradually introduce weight bearing knee flexion activities including a limited number of squats but no single leg squats or lunges until approved by your surgeon. Take great care to increase activity only very slowly. It is important that there is good continued liaison between your Surgeon and Physiotherapist.
Assessment of results of repair:
MRI scans are not a very reliable guide to the success of repair as the resolution of the scans cannot pick up the difference between healing tissue and degenerative material within the meniscus until quite a long time has elapsed following surgery. Even then the images need to be interpreted with quite a lot of caution.
Arthroscopic review is much more accurate but is really not needed in most cases and usually the best way of managing things is to take a pragmatic approach gradually increasing exercise after 3-6 months and seeing how the knee behaves.
If the tear has actually healed then the likelihood is that the patient will be able to resume activities. If not then at some stage a further arthroscopy will prove necessary.
Options during surgery:
It is important to realise that at surgery there will be different options available depending on which part of the meniscus is involved and how severe is the tear. Most cases are treated by conservative trimming of the meniscus. However where there is a large peripheral tear there is a potential to undertake a repair. In many cases there is a combination of judicious trimming together with a repair of the most readily treatable part of the tear.
In recent years attempts have been made to create artificial materials to insert instead of the meniscus but these materials are still at a relatively early stage of development.
The use of meniscal transplant using a cadaveric meniscus is also something to be be considered especially in a relatively young person in whom most or all of the meniscus has had to be removed. These are highly specialised operations and relatively few surgeons in the UK perform them. We currently do not carry out this type of surgery at London Knee Clinic.
TEXT Copyright London Knee Clinic 2014