ACL reconstruction
When the ACL ruptures unfortunately it’s impossible to pull the ends back together. It’s such a short ligament in quite a confined space and there just isn’t any slack or room to do an in-substance repair. The only sensible way to proceed is to remove the frayed ends and replace the ligament with new tissue. The only exception to the above is where the ACL itself remains intact and pulls away a chunk of bone from the tibia. This sometime happens in children and adolescents. In this situation you can replace the piece of bone and fix it back into place. As the ligament is still in one piece function is restored.
|

|

|
|
Intact ACL
|
Torn ACL
|
How ACL reconstruction is performed
The operation of ACL reconstruction involves a number of steps:
-
The knee is examined by arthroscopy to check for any damage to the menisci or articular surfaces
-
The old fragments of ruptured ACL are removed and the size of the intercondylar notch where the ACL runs is assessed
-
If necessary the notch is enlarged – notchplasty
-
The hamstring tendons known as gracilis and semitendinosus are removed to use as graft material. Alternatives include using the central part of the patellar tendon, or an allograft (cadaveric donor tendon) can be used
-
A guide wire is drilled into the tibia and over this is placed a hollow drill to create a tunnel corresponding in diameter to the tendon graft on average 7 to 8 mm in diameter
-
A guide wire is then passed into the femur and a 4 mm hollow drill goes over the guide wire and through the tibia and removed. Part of the femoral tunnel is now over-drilled with a hollow 7 or 8 mm drill but this stops short of penetrating the upper femur
-
Suture material is threaded through the tunnels with the tendon graft attached.
-
The graft is then pulled into position and the ends firmly fixed using various forms of fixation such as resorbable screws.
|
|
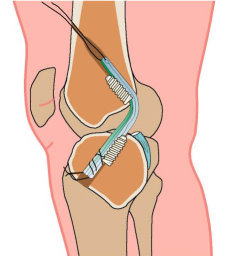
Side view of the knee
The ACL graft (blue) is shown
in the tibial and femoral tunnels and
held in position by resorbable screws
|
|
|
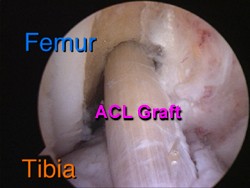
Direct frontal view
Showing the ACL graft
as seen at arthroscopy
|
Rehabilitation after ACL reconstruction
Post-operative rehabilitation starts in the immediate postoperative period when the leg is placed is a continuous passive motion machine. This achieves two things: elevation, important to minimise swelling, and early mobility, which prevents stiffness. Pain relief in the post-operative period is provided by a femoral nerve injection given at the time of surgery, which blocks pain. A disadvantage of the block is that it also leads to muscle weakness. It takes about 24 hours for the block to wear off hence the use of continuous massive movement during that period.
After 24 hours most patients are able to get up and about with crutches and some go home on the day after surgery. Others take a little longer and go home on the second day. A knee brace is not usually required as the graft is sufficiently strong
There is always some variation from one patient to another regarding the speed of rehabilitation and to some extent this depends on age and general fitness and body weight. It also depends on whether other procedures have been required along with the ACL reconstruction such as meniscal repair or cartilage surgery.
Standard rehabilitation regime
-
Day 1 to Week 6: Full weight bearing is resumed as soon as possible and initially between 2 crutches. The crutches are discarded by week 2. Range of movement exercises. Muscle strengthening. Propriocetive training. Closed chain exercises. No hopping, skipping, jumping or running.
-
Week 6 to Week 12: Depending on progress open chain exercises are introduced and light jogging allowed if surgeon permits. No sport yet.
-
Up to 9 months: Intensive muscle strengthening, proprioceptive training and beginning of sport-specific training.
-
From 9 months: Careful return to competitive sport when surgeon permits.
The importance of a slow return to sporting activities
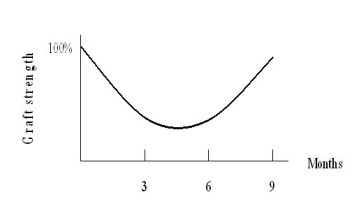
It is important to realise that the tendon used as the graft for the ACL is removed from its blood supply before being reinserted. New blood vessels then grow into the tendon re-establishing a blood supply. The vessels bring in new cells which gradually replace the collagen of the tendon with new fibres. As a result of this process the graft becomes gradually weaker with a danger period between 3 and 6 months when it is more prone to stretch. It takes 9 months to get back to full strength.
|
|
|
Strength of the ACL graft over time
The danger of stretching is greatest between 3 and 6 months
|
TEXT Copyright London Knee Clinic® 2014