Total Knee Replacement (TKR) has evolved over many years and now most cases involve resurfacing of the ends of the bone after removal of a relatively section of bone, around 9mm from the end of the femur, the top of the tibia and the deep surface of the patella. These surfaces are then clad in metal components, these days often with a ceramic surface on the femoral component and with a plastic or high density polyethylene bearing between the tibia and the femur. The deep surface of the patella is generally also resurfaced with a polyethylene bearing.
TKR is quite a major procedure, normally undertaken under general anaesthesia. The operation surgery generally takes somewhere in the region of 2 hours from induction of anaesthesia to return to the recovery room. It normally requires a hospital stay of about 5 days depending on progress and takes up to 3 months for the muscles around the knee to recover fully and for patients to feel the real benefits of surgery.
|

|
Osteoarthritiis right knee as seen on x-ray
|
|

|
A typical total condylar knee replacement
|
|

|
Plastic bone model showing knee replacement in place
|
|
|
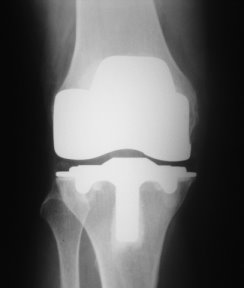
X-ray of a Total Knee Replacement seen from the front
|
|

|
Seen from the side
|
ANIMATION
Results
About 95% of patients have a very good or excellent functional outcome following TKR with the majority remaining very satisfactory for 10-15 years. However it is important not to expect too much. Most patients having a total knee have low functional demands and they are not designed for people continuing in sporting activities. Indeed in the younger very active patients they are prone to earlier failure leading to revision being required rather more rapidly than in older patients.
Potential complications
The commonest complications of TKR are:
Infection
Infection rates vary and at London Bridge Hospital published infection rates are of the order of 1 in 1000. The causes of infection are bacteria carried in the air, and on the surface of our skin and very generally in our environment. Even though surgery is done in an ultra clean air operating theatre and with all sterile precautions in place there is still a small risk of bacteria getting into a knee at the time of surgery. All patients are given a short course of antibiotics to help control this risk.
Superficial infections often resolve with antibiotics treatment. However deep infections can be very serious, as the bacteria can be very difficult to eradicate from the surface of the metal components of the knee replacement. In many cases the only way of getting rid of such infections is to completely revise the knee replacement.
Thromboembolism
Blood clots in the leg otherwise known as deep vein thrombosis or DVT, is a significant risk after a total knee replacement. Small DVTs are common and often cause little or no symptoms. However larger DVTs can cause painful swelling of the leg, with a risk of clots breaking off and travelling into the chest, a so called Pulmonary Embolism or PE. This is a very serious complication and causes chest pain, shortness of breath and in some cases can prove fatal.
To reduce the risk of DVT we encourage our patients to move their legs and walk as soon as possible after surgery. In addition, most patients are given subcutaneous low molecular weight heparin (LMWH) into the skin once daily starting shortly after surgery. This thins the blood and reduces the risk of DVT. The downside is an increased risk of bleeding.
Ultrasound scans are used to moinitor for DVTs in the post-operative period and if detected patients are generally started on Warfarin which may need to be continued for three months post surgery.
Other surgical options
In patients in whom the knee is out of alignment an osteotomy, which involves cutting and straightening the bone either above or below the knee, is ofetn suggested especially in younger patients. This can improve pain to a great extent and defer or eliminate the need for knee replacement surgery.
TEXT Copyright London Knee Clinic® 2014